
 Javier Escaned (Hospital Universitario Clínico San Carlos, Madrid, Spain) discusses the increased interest in coronary microcirculation and non-obstructive coronary artery disease.
Javier Escaned (Hospital Universitario Clínico San Carlos, Madrid, Spain) discusses the increased interest in coronary microcirculation and non-obstructive coronary artery disease.
Why is there recent interest in coronary microcirculation and non-obstructive coronary artery disease?
For the first time, there is a general awareness among cardiologists that angina may have a non-obstructive origin. There are now tools available for diagnosis and effective treatments, and there is evidence that the quality of life of these patients can be significantly improved. The evidence has been so compelling, that it has been included in the 2019 European Society of Cardiology (ESC) Clinical Practice Guidelines on Chronic Coronary Syndromes, which provides recommendations on angina caused by coronary microcirculatory dysfunction (CMD).
Why has this not previously been the case?
Due to the relevance of coronary angiography as a diagnostic tool, ischaemic heart disease largely remained a stenosis-centred condition. New imaging developments, like computed tomography (CT) angiography, focused on the diagnosis of coronary stenosis, and physiology indices like fractional flow reserve (FFR) were not an exception: they did not inform on the presence of CMD, only about the functional relevance of the stenosis. These developments were phenomenal but kept coronary stenosis as the centre of the problem. Finally, many interventionalists adopted a therapeutic nihilist attitude: “I can treat a stenosis, but I can not treat microvascular dysfunction: why should I care?” Additionally, there were not many specific diagnostic tools for CMD broadly available, but that is changing.
What is CMD? What are the clinical subsets to consider?
Microcirculatory dysfunction is a wide term that indicates that one or more roles of the coronary microcirculation are not fulfilled. From a practical perspective, the term is too vague: there are multiple pathways of dysfunction, each requiring a specific test and, subsequently, a specific approach. In patients with chronic coronary syndromes the two main CMD endotypes are structural remodelling of the microvasculature and vasomotor disorders with an origin in endothelial or smooth muscle cell dysfunction.
How does CMD affect patients?
It is a frequent cause of anginal symptoms and an impaired quality of life that can be substantially improved if a CMD endotype is identified and followed by stratified treatment. Studies performing a longitudinal follow-up of patients with objective evidence of CMD have demonstrated that it has major prognostic implications. At a difference of symptoms, it is still unclear if the prognostic implications of CMD can be modified by specific treatment.
Do you need invasive studies, or can you rely on non-invasive testing?
PET-based measurement of coronary blood flow is the best non-invasive approach to diagnose CMD, but, it is seldom available. Methods based on abnormal LV segment performance may not detect globally distributed CMD. Of note, as acetylcholine testing is contraindicated in non-invasive tests, vasomotor disorders cannot be explored and identification of CMD is limited to the structural endotype. The advantage of intracoronary testing is that it constitutes a one-stop-shop to explore the relevance of intermediate stenoses, explore vasomotor tone with acetylcholine, and rule out structural microcirculatory abnormalities.
What information can you obtain to diagnose CMD with PressureWire X (Abbott)?
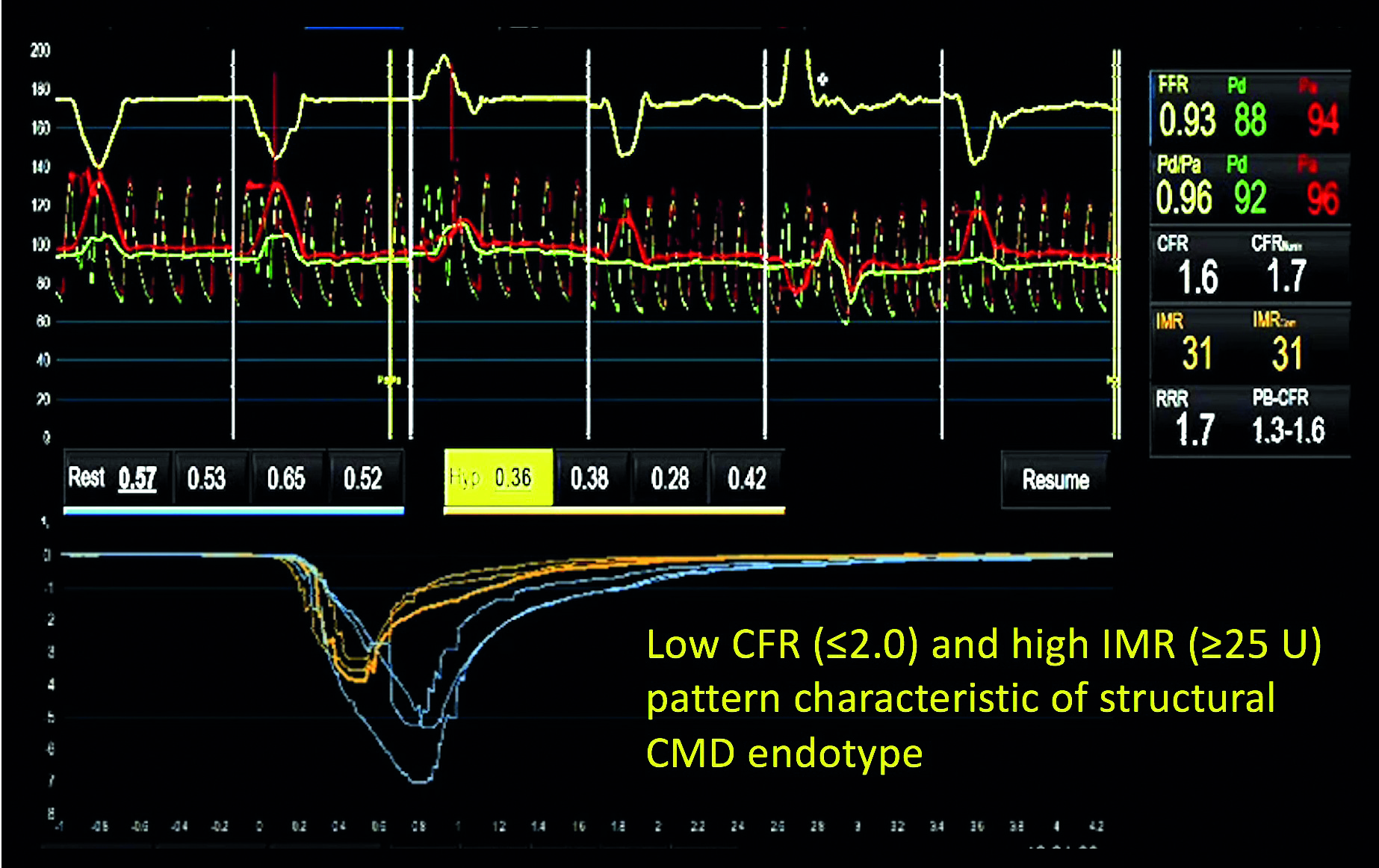
The PressureWire X is fitted with a sensor that measures both intracoronary pressure and temperature. It can be used in patients with angiographically normal arteries or with coronary stenoses. The diagnosis of structural CMD with the PressureWire X is based on the measurement of coronary flow reserve (CFR) and the index of microcirculatory resistance (IMR). An estimate of coronary flow, mean transit time (Tmn), is obtained using the thermodilution principle by performing saline injections from the guiding catheter while the pressure wire is inside the vessel. For CFR, measurements of Tmn are obtained at rest and during maximal hyperaemia. For IMR, only the hyperaemic Tmn and the intracoronary pressure are used for the calculation. Abnormal values are CFR≤2.0 and IMR≥25 units. (Figure 1) Finally, the diagnosis of a vasomotor CMD endotype is based on the administration of intracoronary acetylcholine to assess the presence of endothelial dysfunction and epicardial spasm. Electrocardiogram (ECG) monitoring and repeated angiograms after each acetylcholine dose are required to assess the development of ischaemia, overt epicardial spasm, and changes in vessel diameter or TIMI flow.
What is the value of the Coroventis system (Abbott)?
The Coroventis system is a dedicated console that establishes a wireless connection with the PressureWire X. It allows you to diagnose epicardial disease and microvascular dysfunction in a single system. In addition to calculating FFR and RFR, it calculates CFR and IMR from the thermodilution and pressure data, either as outlined above and alsoor through alternative methods, like using a continued infusion of saline through a dedicated microcatheter. Currently, the Coroventis system is an indispensable element in using the PressureWire X to assess CMD. (Figure 1)
How do you integrate information obtained to clinical management of the patient?
In the structural CMD endotype, betablockers, are the first choice to control angina. In the vasomotor CMD endotype and epicardial spasm, calcium channel blockers and nitrates are used to control symptoms. In both CMD endotypes, statins, ACE inhibitors, control of cardiovascular risk factors and changes in lifestyle are recommended.
What are the next steps in this field?
There is evidence that assessment of the microcirculation downstream the culprit vessels of ST-elevation myocardial infarction (STEMI) informs on the presence of the so-called microvascular obstruction phenomenon (MVO). It is foreseeable that in the near future patients with high IMR after successful primary PCI will be managed with specific treatments that aims to reduce this acute form of CMD.
Reference
1 de Waha S, Patel M, Granger CB, et al. Relationship between microvascular obstruction and adverse events following primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: an individual patient data pooled analysis from seven randomized trials. Eur Heart J 2017; 38(47): 3502–3510.
Disclosure
Javier Escaned has been issued consultancy fees from Abbott.









