

Transcatheter aortic valve implantation (TAVI) is now a well-established treatment for aortic stenosis and is approved as an alternative to surgical aortic valve replacement in high-risk and intermediate-risk patients. Increasingly, the transcatheter heart valves are also being used for novel applications when conventional treatments are either not possible or considered too high risk. One such application has been valve-in-valve therapy. During a valve-in-valve procedure, a transcatheter heart valve is implanted within a failing bioprosthetic surgical heart valve. In this commentary, Vratika Agarwal and Vinayak Bapat discuss the need to consider future valve-in-valve procedures when implanting a surgical valve.
In early experiences, the outcome of TAVI valve-in-valve procedures has been excellent and has added advantages vs. redo surgical procedures—such as short procedure time and less invasive procedure; hence, early recovery. Initially, only failing aortic surgical heart valves were treated with this technique but now the experience has expanded to structurally deteriorated surgical heart valves in the mitral, tricuspid and pulmonic position. Additionally, failed mitral or tricuspid valve repairs with annuloplasty rings can now be treated with a valve-in-ring procedure, whereby the transcatheter heart valve is implanted and anchored within a mitral ring.
As with any other treatment, the initial experience has been in carefully selected high-risk patients, but now most patients are considered for a valve-in-valve or valve-in-ring option. This will become increasingly relevant soon as, in the Western world, the majority of the patients prefer a biological valve and age cutoff for mechanical vs. biological valve can be as low as 50 years. The main premise of considering valve-in-valve is to avoid another open-heart surgery. However, achieving a good long-term result is of paramount importance. Thus, understanding the limitations of valve-in-valve and valve-in-ring are essential to help prepare a platform conducive to a future transcatheter option.
The need to be TAVI friendly
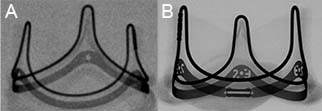
One of the main issues associated with valve-in-valve therapy is the “Russian Doll” effect. As the transcatheter heart valve is implanted within a pre-existing surgical heart valve, its expansion and its function is entirely dependent on the “internal diameter” of the surgical valve. Literature has shown that smaller surgical valves have worse long-term results. Hence, one solution is expansion of the surgical heart valve size by using certain surgical techniques. Another common issue is proper identification of the degenerated surgical heart valve, i.e. type and size. Fortunately, most surgical valves have a unique footprint when visualised under fluoroscopy and type of surgical heart valve can be readily identified, but not size. Size of the surgical heart valve is the most critical piece of information as it dictates the size of transcatheter heart valve. Measurements of the surgical heart valve with computed tomography (CT) and echocardiography are not standardised and can lead to an error. A surgical heart valve with size markers allows for the valve size to be identified easily under X-ray and is highly beneficial. Design modifications of the new generation surgical heart valve that allow for future implantation of transcatheter heart valve when chosen during the first surgery can make valve-in-valve procedure at a later date easy to plan and execute. One of the first surgical heart valve designed to be TAVI friendly has been the Edwards Lifesciences Inspiris (Edwards Lifesciences) pericardial valve (Figure 1). This surgical heart valve has a possibility of expansion of the basal band, which results in an increase in the stent internal diameter. We are bound to see more and more of valves that are designed to adapt to this idea.
There are certain scenarios in which modified surgical techniques can have a huge impact on the feasibility of valve-in-valve/valve-in-ring at future date. One such scenario is a surgical patient with small aortic annular dimensions. Implanting a small sized valve during the first surgery makes the future vavle-in-valve result suboptimal. Hence, procedures such as a “Root enlargement” should be performed to implant a larger surgical heart valve. This is especially important in younger patients who choose a bioprosthetic surgical heart valve, as their likelihood of outliving the surgical heart valve life is high and re-intervention is near certain. Another scenario in which surgical techniques can be modified is radio-opaque marking of the annulus after stentless valve implantation. This allows for visualisation of the valve during future procedures. These changes in surgical practice were initially slow but have since increased with growing participation of surgeons in the transcatheter field.

With the increased use of transcatheter heart valve within failed mitral bioprosthetic surgical heart valve and rings as valve-in-valve/valve-in-ring approach, some unique problems have come to attention. One of them is the suboptimal result of valve-in-ring when compared with valve-in-valve. Surgical mitral rings are of various types and vary in their construct and design. They can be:
- Rigid, semi-rigid or flexible
- Complete or incomplete
- And can vary in degree of visibility under fluoroscopy.
Of the 20 commercially available implantable rings, only nine rings are TAVI friendly as they can adapt a near-circular shape and can provide a secure anchor to the transcatheter heart valve (Figure 2). Studies have shown favourable results with the use of TAVI friendly rings. Thus the question, can surgeons implant a ring that is TAVI friendly rather than one that is not during mitral valve repair surgery?
Increasing awareness is the key to future transcatheter heart valve success.
Conclusion
To be able to use the transcatheter heart valve to their fullest potential as a future strategy, modification of surgical technique at the time of first open heart surgery and design adjustments of the surgical valves and rings to accommodate transcatheter heart valve devices will prove to be critical.
Vratika Agarwal and Vinayak Bapat is at New York Presbyterian/Columbia University Medical Center, New York, USA. Bapat talked about this topic at the European Association European Association for Cardio-Thoracic Surgery (EACTS) annual meeting (18–20 October, Milan, Italy).









