
 Reduced coronary blood flow, measured using an artificial intelligence (AI)-based tool that analyses imaging from coronary computed tomography angiography (CCTA), may predict future cardiovascular events in patients with suspected stable coronary artery disease.
Reduced coronary blood flow, measured using an artificial intelligence (AI)-based tool that analyses imaging from coronary computed tomography angiography (CCTA), may predict future cardiovascular events in patients with suspected stable coronary artery disease.
These are among the findings of analysis from the FISH&CHIPS study, a retrospective study of more than 90,000 patients conducted by the NHS in England, presented at the congress of the European Association of Cardiovascular Imaging (EACVI; 11–13 December, Vienna, Austria).
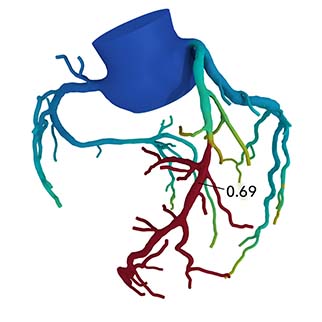
CCTA is a non-invasive heart scan that is used as the first-line investigation for patients with suspected stable coronary artery disease (CAD). While CCTA clearly shows blockages in coronary arteries, it is limited in its ability to estimate reduced blood flow, which is necessary to diagnose angina. CT-derived fractional flow reserve (FFR-CT, Heartflow) uses computational fluid dynamics analysis of coronary blood flow obtained from CCTA images to estimate the decrease in pressure across coronary stenosis during the maximum hyperaemia.
The real-world, retrospective, nationwide FISH&CHIPS study demonstrated that including FFR-CT as a decision-making tool in the diagnosis of stable CAD reduces the number of subsequent invasive and non-invasive tests performed.
“We already know that FFR-CT is valuable for the diagnosis of stable CAD, but whether FFR-CT could also be used prognostically, to predict future major cardiovascular events, is not fully understood,” explained study presenter, Jack Bell (Liverpool Heart and Chest Hospital, Liverpool, UK). “Previous studies have had small patient numbers, short follow-up and investigated combined cardiovascular outcomes. We performed an analysis from a national FISH&CHIPS population, which was large enough to determine whether FFR-CT adds incremental value to traditional cardiovascular risk factors in predicting cardiovascular outcomes and death.”
Data from all patients receiving FFR-CT analysis for stable CAD at 27 English sites in the FISH&CHIPS observational cohort study were included in the presented analysis. FFR-CT measurements were related to the individual outcomes of myocardial infarction (MI), cardiovascular mortality, all-cause mortality and whether the patient underwent subsequent revascularisation (coronary artery bypass grafting or stenting). FFR-CT measurements were divided into subgroups: normal (FFR-CT >0.8), borderline (0.71–0.8), reduced (0.51–0.7) and severely reduced (≤0.5).
Of 90,553 patients receiving CCTA, 7,836 patients underwent FFR-CT. They had a median age of 63 years and 37.4% were female. At a median follow up of 3.1 years, there were 191 MIs (2.4%), 1,573 revascularisations (20.1%), 74 cardiovascular deaths (0.9%) and 261 all-cause deaths (3.3%).
When FFR-CT was measured close to the stenosis (blockage) site, lower values were associated with higher cardiovascular event rates: FFR-CT categories incrementally stratified risk of MI (p<0.001), revascularisation (p<0.001), cardiovascular mortality (p<0.001) and all-cause mortality (p=0.002) over time. As an example, MI occurred in 1.0% of patients with normal FFR-CT, 2% of patients with borderline FFR-CT, 3.9% of those with reduced FFR-CT and 5.2% of those with severely reduced FFR-CT.
Patients with the lowest FFR-CT values had a four-fold increased risk of a heart attack and a threefold increased risk of dying from a heart attack. FFR-CT less than normal was associated with an increased risk for future MI and revascularisation, with severely reduced FFR-CT also associated with cardiovascular death and death. This was independent of traditional cardiovascular risk factors such as age, sex, hypertension, diabetes and dyslipidaemia.
Senior author, Timothy Fairbairn (Liverpool Heart and Chest Hospital, Liverpool, UK), said: “Adding to its diagnostic abilities, this study is the first to provide conclusive evidence of FFR-CT’s prognostic power, independent of other risk factors. We observed that even so-called ‘borderline’ FFR-CT was associated with worse outcomes compared with normal values, but the individuals with the lowest values have the highest risk. FFR-CT could be used to inform personalised risk assessment, allowing us to provide more intensive bespoke treatment to those at high risk.”
Results of an analysis investigating the cost-effectiveness of using FFR-CT in the diagnosis of stable CAD will also be presented at EACVI 2025.






