
 A pilot randomised trial of percutaneous coronary intervention (PCI) of non-flow-limiting vulnerable plaques in native coronary arteries—PROSPECT ABSORB—has found that PCI is safe, substantially enlarges follow-up lumen areas, and is associated with favourable long-term clinical outcomes. The findings were presented during a late breaking trial session on the first morning of TCT Connect 2020 (14–18 October, virtual) by Gregg Stone (Icahn School of Medicine, Mount Sinai, New York, USA), and published simultaneously in the Journal of the American College of Cardiology.
A pilot randomised trial of percutaneous coronary intervention (PCI) of non-flow-limiting vulnerable plaques in native coronary arteries—PROSPECT ABSORB—has found that PCI is safe, substantially enlarges follow-up lumen areas, and is associated with favourable long-term clinical outcomes. The findings were presented during a late breaking trial session on the first morning of TCT Connect 2020 (14–18 October, virtual) by Gregg Stone (Icahn School of Medicine, Mount Sinai, New York, USA), and published simultaneously in the Journal of the American College of Cardiology.
PROSPECT ABSORB was an investigator-sponsored, multicentre, single-blinded, active-treatment-controlled randomised trial that was embedded into the PROSPECT II natural history study. Between June 10, 2014 and December 20, 2017, 902 patients at 16 sites were enrolled in PROSPECT II, which sought to validate the use of near-infrared spectroscopy (NIRS) and intravascular ultrasound (IVUS) imaging in identifying non-obstructive lipid-rich plaques that are prone to cause future cardiac events. Data from the PROSPECT II study were also presented during the late breaking trial session.
Outlining the rationale for PROSPECT ABSORB, Stone reported that acute coronary syndromes (ACSs) commonly arise from plaque rupture and thrombosis of coronary artery lesions that angiographically appear mild, but pathologically contain large plaque burden (PB) with an organised lipid-rich necrotic core that is separated from the lumen by a thin fibrous cap. Known as vulnerable plaques, these thin-cap fibroatheromas place patients at risk for future adverse events, including acute myocardial infarction (MI) and cardiac death. Vulnerable plaques may be identified by several imaging techniques.
During the study, three-vessel imaging was performed with a combination IVUS and NIRS catheter after successful PCI of all flow-limiting coronary lesions in 898 patients presenting with MI. Among these, 182 patients at 15 centres with an angiographically non-obstructive stenosis not intended for PCI but with IVUS plaque burden ≥65% were randomised to treatment of the lesion with an Absorb (Abbott) bioresorbable vascular scaffold (BVS) plus guideline-directed medical therapy (GDMT) (n=93) vs. GDMT alone (n=89).
The primary effectiveness endpoint was the IVUS-derived minimum lumen area (MLA) at protocol-driven 25-month follow-up. The primary (non-powered) safety endpoint was target lesion failure (TLF; composite of cardiac death, target vessel-related MI or clinically driven target lesion revascularisation) at 24 months. Angiographic follow-up at 25 months was completed in 167 patients (91.8%), and median clinical follow-up was 4.1 years.
The follow-up MLA in BVS-treated lesions was 6.9±2.6mm2 compared with 3.0±1.0mm2 in GDMT-alone-treated lesions (least square means difference 3.9mm2, 95% CI 3.3-4.5, p<0.0001). TLF at 24 months occurred in similar rates of BVS-treated and GDMT alone-treated patients (4.3% vs. 4.5%; p=0.96). The secondary (non-powered) clinical effectiveness endpoint of randomised lesion-related MACE to the time of latest follow-up occurred in 4.3% BVS-treated patients vs. 10.7% GDMT-alone-treated patients (OR 0.38, 95% CI 0.11‒1.28, p=0.12).
“The results from PROSPECT ABSORB indicate that PCI of vulnerable plaques may safely enlarge the lumen and change the structure of the lesion, theoretically reducing its propensity for thrombosis and progression,” said Stone, who served as study co-chair alongside David Erlinge (Lund University, Lund, Sweden).
“The favourable randomised lesion-related MACE rates observed after BVS treatment compared with medical therapy alone warrants the performance of an adequately powered randomised trial to determine whether PCI treatment of vulnerable plaques improves patient outcomes.”
 Earlier in the session, Erlinge presented data from the PROSPECT II study which found that NIRS-IVUS intracoronary imaging could be a useful tool in identifying angiographically non-obstructive lesions with high-risk characteristics for future adverse cardiac outcomes. According to Erlinge, recent studies have suggested that lipid-rich plaques detected by intracoronary NIRS imaging are associated with adverse outcomes, and identifying these vulnerable plaques before they progress may help to inform pharmacologic or other strategies to stabilise the plaque.
Earlier in the session, Erlinge presented data from the PROSPECT II study which found that NIRS-IVUS intracoronary imaging could be a useful tool in identifying angiographically non-obstructive lesions with high-risk characteristics for future adverse cardiac outcomes. According to Erlinge, recent studies have suggested that lipid-rich plaques detected by intracoronary NIRS imaging are associated with adverse outcomes, and identifying these vulnerable plaques before they progress may help to inform pharmacologic or other strategies to stabilise the plaque.
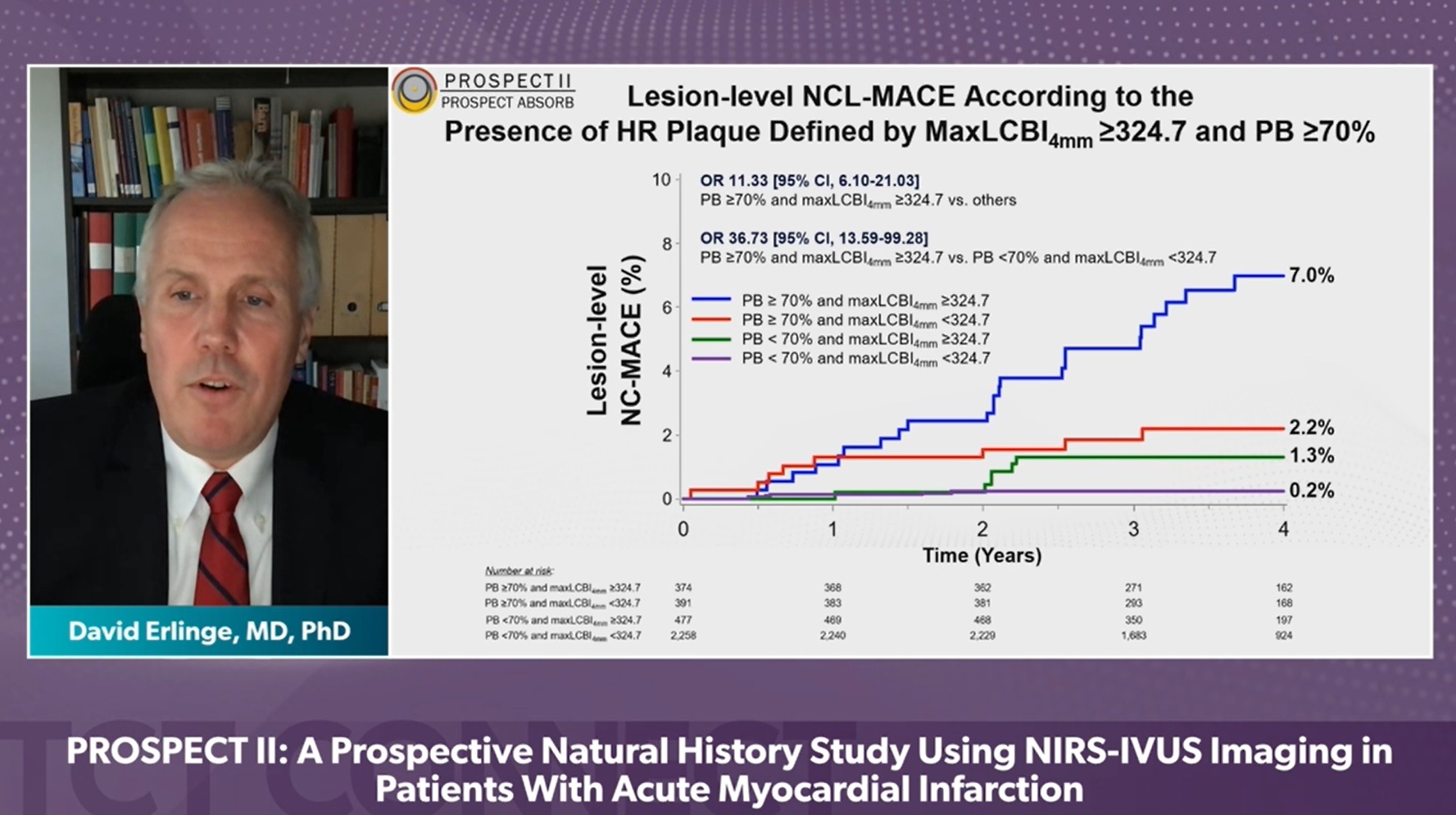
PROSPECT II involved imaging of all three coronary arteries using a combination NIRS-IVUS catheter in patients with recent myocardial infarction who had undergone successful treatment of all flow-limiting lesions. The lipid content of non-culprit lesions was assessed by NIRS, and IVUS assessment was also performed. The primary outcome was the covariate-adjusted rate of major adverse cardiac events (the composite of cardiac death, myocardial infarction, unstable angina, or progressive angina) adjudicated to have arisen from non-culprit lesions. The relationship between plaques with high lipid content, large plaque burden, and small lumen areas and patient-level and lesion-level events were tested hierarchically.
A total of 3,629 untreated non-culprit lesions were prospectively characterised in 898 patients with myocardial infarction. Adverse events within four years occurred in 13.2% of patients, with a total of 8% of events arising from untreated non-culprit lesions with a mean baseline diameter stenosis of 46.9%. The presence of highly-lipidic lesions was an independent predictor of patient-level non-culprit events (adjusted OR 2.27; 95% CI 1.25‒4.13) and lesion-specific events (adjusted OR 7.83; 95% CI 4.12‒14.89). Large plaque burden and small lumen areas were also independent predictors of adverse events, the study team found.
“In PROSPECT II, lipid-rich plaques, as detected by NIRS, identified angiographically mild non-flow limiting lesions responsible for future coronary events,” said Erlinge. “High lipid content, along with large plaque burden and small lumen area, may be added as prognostic indices of vulnerable plaques that put patients at risk for adverse outcomes. Further studies prospectively utilising this information are warranted to improve outcomes for high-risk patients with coronary artery disease.”
The PROSPECT II trial was funded by research grants from Abbott Vascular, Infraredx and The Medicines Company.








