

SyncVision (Philips Volcano) enables co-registration between angiogram and intravascular ultrasound (IVUS) images during percutaneous coronary intervention (PCI). Following recent CE mark and FDA clearance the technology can also be used in tandem with instant wave-free ratio (iFR, Philips Volcano) assessment. In this article, Cardiovascular News reviews how SyncVision with iFR co-registration may be able to help optimise procedural outcomes.
In a 2008 study of patients undergoing PCI with a sirolimus-eluting stent, Costa et al1 found that a suboptimal PCI result—in the form of geographic miss—was not only a common occurrence (observed among 66.5% of patients) but also was associated with worse long-term outcomes. The authors report that at one year, patients with geographic miss had a significantly higher one-year rate of target vessel revascularisation. Furthermore, they found that geographic miss was associated with a three-fold increased risk of myocardial infarction. “The results emphasised the need for improvement in contemporary PCI practices and technologies,” Costa et al conclude.
Iqbal Malik (Imperial College, London, UK) views IVUS as a key technology, which should be used to improve PCI procedural outcomes by optimising stent expansion and apposition. He believes that one of the main reasons why, according to his estimates, 20–30% of procedures are suboptimal in current practice is the lack of use of IVUS. Malik notes that operators may incorrectly size a vessel if they only use angiography, commenting: “If I ever needed a stent and the operator did not use IVUS to ensure that the stent was perfectly placed, I would ask them why not afterwards. I use IVUS for the majority of my patients, particularly if I was putting a stent in the left main. That area is well known for being difficult to stent correctly.”
Several studies do support the use of IVUS-guided PCI. For example, in a meta-analysis, Elgendy et al2 found that IVUS-guided PCI for patients with diffuse lesions was associated with a significant increase in postdilation compared with angiogram-guided PCI: 63% vs. 47% (p<0.0001). They also found that IVUS-guided PCI was associated with a significant reduction in the risk of major adverse cardiac events (6.5% vs. 10.3% for angiogram-guided PCI; p<0.0001). Reporting that this finding was “mainly because of reduction in the risk of ischaemia-driven target lesion revascularisation”, the authors conclude: “The routine use of IVUS for revascularisation of diffuse coronary lesion should be considered.”
However while IVUS may help to optimise outcomes, matching up the IVUS image with the angiogram image can be challenging. Malik explains: “Until recently, it was quite difficult because you had to have your eyes on one screen for one bit of data and on another screen for another bit of data.” SyncVision is designed to address this challenge because it co-registers the angiogram and IVUS images, meaning the operator can see them on one screen.
Justin Davies (Imperial College, London, UK) notes that a benefit of the technology is that operators do not need to perform automated pullback. He explains that pullback is needed when the whole of the vessel has to be assessed, commenting: “You cannot keep the IVUS catheter static; you need to pull it back. But with SyncVision co-registration, because the IVUS and angiogram images are combined, you can track the position of the catheter on the X-ray as you manually pull it back.” Malik adds that this feature helps operators to determine the length of the lesion and, therefore, “you hopefully do not underestimate or overestimate the length of the lesion; thus, you choose the correct length of stent.”
Having used the technology quite a few times, Malik says he finds it “intuitive”. “Once you have used SyncVision a couple of times, what you to need to click to get to the next step is quite obvious. Therefore, it is operator friendly.”
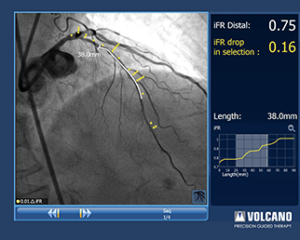
A new feature of SyncVision, following CE mark and FDA clearance, is that it can now be used to co-register iFR values to the angiogram for complete physiological assessment.
iFR is used to assess the functional significance of a stenosis during the wave-free period when resistance is naturally constant and minimised during the cardiac cycle. The ADVISE II study,3 which was sponsored by Volcano (now Philips Volcano), found that a pre-specified iFR cut-off of 0.89 correctly classified 82.5% of stenoses with a sensitivity of 73% and specificity of 87.8%. Furthermore, authors Escaned et al report that using a hybrid iFR and fractional flow reserve (FFR) approach—treat lesions ≤0.85, use FFR for lesions with iFR 0.86–0.93, and defer treatment for lesions with an iFR ≥0.94—“obviated vasodilators from 65.1% of patients and 69.1% of stenoses”.
iFR does not require the use of hyperaemic agents such as adenosine. This may be better for patients in whom hyperaemic agents are contraindicated and may be more cost-effective. Davies comments that not having to use adenosine means that iFR, specifically the iFR Scout software, is a good tool for performing pullback assessment.
Pullback assessment is useful for situations in which the initial physiological assessment indicates that the patient has functionally significant lesions but, as Davies reports, identifying where the most important lesion (ie. in cases of diffuse disease) on the IVUS or angiogram image is “very difficult”.With iFR, the pressure wire is pulled back across the vessel to find the area of greatest ischaemia. Malik explains: “If you perform iFR pullback in a vessel with diffuse disease and there is no focal step-up, then you will have to treat that whole segment to get significant improvement. However, if pullback shows a focal step-up, then localised treatment with a short stent will suffice. The angiogram may look severe but the other lesions in the vessel are not causing a significant problem.”
According to Davies, SyncVision with iFR co-registration provides additional benefits when performing pullback assessments. He says: “For more than 15 years, it has been reported that FFR or other hyperaemic measures are fundamentally limited in serial lesion assessment because of cross talk between lesions. Using resting values of iFR makes it possible to interpret them in a simple and reliable manner. iFR co-registration with SyncVision takes this to the next stage as it allows the location of iFR pressure drops to be easily mapped onto the angiogram. This enables the interventionalist to easily pinpoint where to deploy a stent and to easily differentiate between focal and diffuse disease.”
Davies explains that the iFR pressure loss is “very shallow” in diffuse disease because the energy loss occurs “at a slow pace” but iFR pressure loss is steep with focal disease because “the energy loss occurs rapidly over a narrow segment of vessel”. “iFR co-registration offers the potential to be able to map these diffuse and focal lesions onto the angiogram to easily identify areas of the vessel to treat which would benefit from PCI maximally,” he adds.
Additionally, pressure wire pullback with iFR Scout produces a physiological map of the entire vessel as a function of time whereas SyncVision with iFR co-registration maps physiological data onto an angiogram as a function of distance.
Both Malik and Davies say that SyncVision with iFR co-registration are useful tools, with Davies calling iFR co-registration “robust, reliable, and very easy to use”. He adds: “Unlike many other co-registration technologies, the iFR co-registration technology only requires images from a single plane. This saves time, contrast and additional radiation exposure. Most importantly it allows us to target the areas for PCI with the most focal energy loss simply and easily.”
Summing up his experience with the SyncVision technology with iFR co-registration, Malik says he finds it works “very effectively”. “iFR helps you to decide if treatment is needed and where that treatment is needed. The IVUS and angiogram co-registration enables you to decide what size of stent you need, what length of stent you need, and review how well the stent is placed.” He adds that it may be particularly useful for stenting the left main, bifurcations, and longer lesions.
This article has been sponsored by Volcano Europe SPRL/BVBA, also trading under the brand name of Philips Volcano. These views expressed are those of the physicians and do not necessarily reflect those of the company or those of Cardiovascular News.
References
- Costa et al. Am Cardiol 2008; 101: 1704–11.
- Elgendy et al. Circ Cardiovasc Interv 2016: Epub.
- Escaned et al. J Am Coll Cardiol Intv 2015; 9: 824–33.









