

This advertorial is sponsored by Medtronic
Due to the growth of transcatheter aortic valve implantation (TAVI) in recent years—initially available to patients at high surgical risk, then more recently to those deemed to be at moderate risk, and now increasingly offered to patients who would be considered at low risk for surgery—the question of valve durability becomes ever more important.
“It is not only important for TAVI, but it is also important for surgical aortic valve replacement [SAVR], because we now speak about low-risk patients, [and] younger patients,” Hendrik Treede (University Hospital Mainz, Mainz, Germany) tells Cardiovascular News.
This focus has changed, Treede acknowledges, as TAVI is now moving towards younger patients—those with a longer life expectancy. From that perspective, he comments, it is highly important to have long-term durability data available for patients who have had TAVI and SAVR, which is seen to be central to the question of which patients may be suitable for a transcatheter valve and which may be more likely to gain benefit from a surgical bioprosthesis. However, the same questions are also relevant when it comes to choosing the appropriate therapy in older and higher risk patients.
“The questions we have to answer today, are ‘what is the journey of the patient?’ and ‘what kind of valve will they have?’,” he notes. “We now speak about patients who will definitely see structural valve deterioration (SVD) during their lifespan. And then the discussion starts on which valve to start with.”
Signals of structural valve deterioration
Understanding the signs and impact of SVD are fundamental to any decision-making process when it comes to setting a strategy for each patient, and predicting whether a transcatheter or surgical approach will give them the greatest benefit. “If you have SVD it means you have irreversible morphological change of the structure of your valve,” says Treede. “That, of course, has an impact on your future life because you may have either aortic stenosis or aortic regurgitation, or even a combination of both. That basically makes you a sick patient again, and you may see all the effects related to it.”
 Morphological changes to the valve, caused by SVD, may be hard to detect, Treede comments, but haemodynamic changes may be more straightforward to identify, and indicative of the presence of SVD. Findings of a study presented at the American College of Cardiology’s annual scientific sessions (ACC 2022, 2–4 April, Washington DC, USA) are among the latest data available that offer some indication of the relative performance of TAVI when it comes to valve durability.
Morphological changes to the valve, caused by SVD, may be hard to detect, Treede comments, but haemodynamic changes may be more straightforward to identify, and indicative of the presence of SVD. Findings of a study presented at the American College of Cardiology’s annual scientific sessions (ACC 2022, 2–4 April, Washington DC, USA) are among the latest data available that offer some indication of the relative performance of TAVI when it comes to valve durability.
The study, a pooled analysis from the CoreValve US Pivotal High Risk and SURTAVI randomised trials, evaluated the five-year incidence and predictors of haemodynamic valve deterioration and clinical outcomes at five years among patients who had been randomised to undergo TAVI—using either the CoreValveTM or EvolutTM (Medtronic) platforms, both supra-annular, self-expanding valves—or SAVR.
For the purposes of the study, investigators defined SVD as moderate or greater haemodynamic valve deterioration, determined as an increase in mean gradient ≥10mmHg from discharge and a mean gradient ≥20mmHg at the last available echo, or the new onset or increase of intraprosthetic aortic regurgitation.
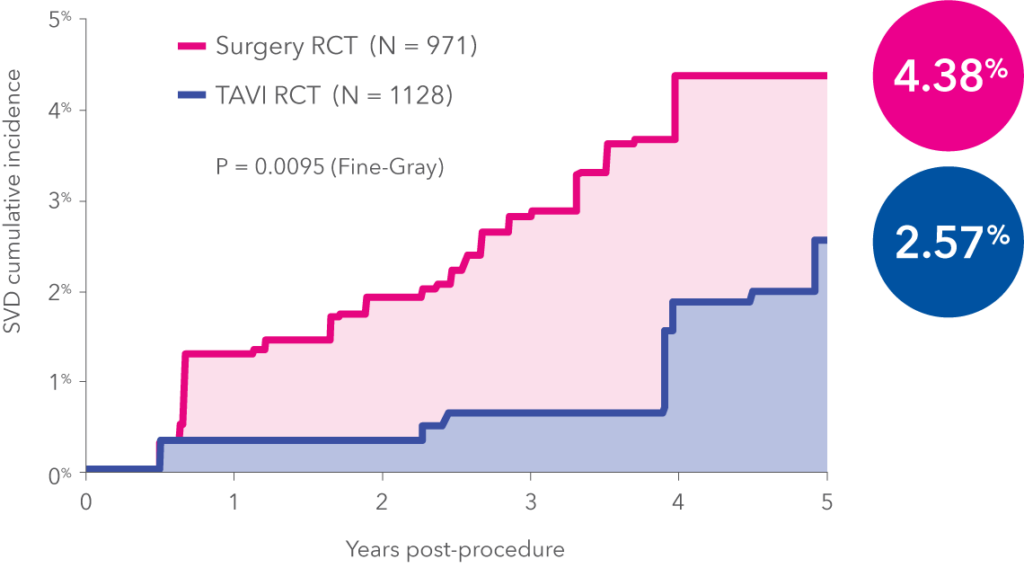
In total, the study evaluated 1,484 intermediate risk (792 TAVI, 692 SAVR) and 615 high risk (336 TAVI, 279 SAVR) for SVD. Headline findings presented at ACC showed that in patients with symptomatic severe aortic stenosis at intermediate or high surgical risk, the five-year rate of SVD was 4.38% in patients undergoing surgery, versus 2.57% in patients undergoing TAVI using the Evolut and CoreValve platforms (p=0.0095). Furthermore, the risk of death and rehospitalisation for aortic valve disease or heart failure doubles in patients that develop SVD, according to the study investigators.
“We know self-expanding valves have larger opening areas due to the supra-annular valve position. It seems very likely that then they may have a longer durability than balloon expandable valves, which sit intra-annular and have, in comparison, higher gradients and smaller, effective opening areas”
Furthermore, the difference in SVD was observed to be more profound in patients with smaller (≤23mm) annuli (5.86% surgery vs. 1.39% TAVI; p=0.049), but a trend was also found in patients with larger (>23 mm) annuli (3.96% surgery vs. 2.48% TAVI; p=0.067).
“It is pretty significant, especially in the light of the use of the very early CoreValve generation at the time,” says Treede, commenting on the data. “That leaves room for the idea that the data might have even been better if they had used the latest generation,” he adds.
Among the important messages to take away from the data are, according to Treede, the fact that there is a low likelihood of developing SVD after five years, and that this may be at least competitive with, and, if not better than surgery. Longer-term follow-up, and more data in lower-risk patients will also be key.
Are all valves created equally?
Could the findings also be extrapolated across the full gamut of devices currently available? Treede suggests possibly not. Asked whether he thinks all valves are equal when it comes to valve durability, he responds: “This is a very important question. It is definitely not true for surgical valves, and we know this, but it may also be different with TAVI valves, because SVD very much depends on haemodynamic function.”
In particular, the use of supra-annular, self-expandable valves may be even more advantageous when it comes to durability than, for example, balloon-expandable valves, Treede goes on to suggest.
“We know self-expanding valves have larger opening areas due to the supra-annular valve position,” he explains. “It seems very likely that then they may have a longer durability than balloon expandable valves, which sit intra-annular and have, in comparison, higher gradients and smaller, effective opening areas.
“So, there is a clue and I think we have some evidence that the durability of certain self-expanding valves might be a bit better than the balloon-expanding valves. But we also have to say that there is no comparative trial with long enough follow-up to really show this in a proper scientific way,” Treede adds.
Returning to the question of lifetime management, Treede acknowledges that the findings of the analysis may have a bearing on the choice of TAVI as a first approach, particularly in younger patients for whom a reintervention may be required further down the line.
“We have to make sure that the second procedure is also safe, and also related to very good long-term outcomes, to speak about TAV-in-TAV options,” Treede comments, adding that, as more younger patients get TAVI as the first choice in many centres, this will be an increasing area of focus.









