

This content is only for readers outside of the US as it discusses a device that is not FDA approved.
The PASCAL repair system (Edwards Lifesciences, Irvine, CA, USA) is a novel leaflet repair therapy. The implant uses clasps and paddles that gently grasp leaflets to facilitate coaptation. The device is implanted via transseptal approach and places a spacer between the valve leaflets to fill the regurgitant orifice.
The CLASP study is a multicentre, multinational, prospective, single-arm study that evaluated the use of the PASCAL repair system for the management of mitral regurgitation (both degenerative and functional). The results from the CLASP study show that the PASCAL repair system is associated with a very important and significant reduction in mitral regurgitation (MR) with 86% of patients having residual MR grade of ≤1+, and 98% of patients with residual MR grade of ≤2+ at 30 days.1
Ulrich Schäfer (Catholic Marienhospital Hamburg, Hamburg, Germany), a CLASP study investigator, explains that CLASP was “a safety and efficacy trial” to “prove the concept” behind the device.
The CLASP study investigators, Lim DS et al, report that the PASCAL repair system paddles “are designed to minimise stress concentration on the native leaflets” and the spacer is “intended to fill the regurgitant orifice area to reduce MR”.1 For Schäfer, these features make the PASCAL repair system “very interesting and innovative” because they are different from those seen with other transcatheter mitral valve repair therapies. He notes that the clasps on the system can be independently adjusted, which enables “a very sophisticated approach to leaflet capture”.

Volker Rudolph (Heart and Diabetes Center, University Clinic, Bad Oeynhausen, Germany) also uses the PASCAL repair system at his centre and, like Schäfer, believes that its unique features may provide several advantages. He comments: “With mitral valve repair, whatever technique you use, you want to achieve maximal leaflet coaptation without impeding forward flow through the valve. I think the PASCAL repair system allows you to reach that goal very efficiently.” In particular, the less rigid, broad nitinol paddles and the central spacer probably help to place less stress on the leaflets while the spacer may reduce the risk of creating an artificial stenosis. Rudolph explains that when you implant a device to repair the mitral valve, you pull the anterior and posterior leaflets together. “If you do this very efficiently, you may create a stenosis which causes the leaflets not to open effectively. However, with a spacer, you are not pulling on the leaflets as much. Therefore, you have more mobility for the leaflets and more residual orifice area. You reduce the leak but maintain movement,” he says.
“The other major aspect that helps optimise coaptation is the separate manoeuvrability of the clasps. This means you can correct the grasping position for the anterior leaflet independent of the posterior leaflet,” Rudolph explains. He adds: “The morphologies of the mitral valve can sometimes be challenging and the forces counteracting on coaptation can only partly be identified from available imaging techniques. Therefore, the ability to do a minor correction of the device by re-grasping just one leaflet with the pliable nitinol paddles is a major advancement that allows an easier optimisation of leaflet coaptation, which often has a significant impact on the procedural result.”
Data from the CLASP study
The CLASP study enrolled 62 patients with MR grade 3+ or 4+ (56% functional, 36% degenerative, and 8% with mixed aetiology). The patients had a mean age of 76.5 years and 51.6% were in New York Heart Association (NYHA) class III or IV.1

At 30 days, of those with a successful implantation (59 patients), 98% of patients had an improvement in MR by one grade or more. This meant that 98% of patients had MR grade ≤2+ and 86% of patients had MR grade ≤1+ (significantly reduced compared with baseline levels, p<0.0001; Figure 1). Schäfer calls these results “remarkable”, noting that the reduction in MR is “very profound”. Another study with MitraClip, COAPT, which only included patients with functional MR, showed 92.7% of patients had MR grade ≤2+ and 72.9% had MR grade ≤1+ at 30 days.1,2 Additionally, Schäfer observes, COAPT was a trial with procedures performed by operators with extensive device experience, whereas CLASP was a trial in which the study investigators had less experience with the device by the nature of the PASCAL repair system being a novel implant. “The COAPT study showed the best-ever published data regarding the success of reducing MR. Now the CLASP study shows very important reductions in MR. I think that these findings of CLASP are very interesting.”
Importantly, successful implantation was achieved in 95% of patients, with an average of 1.5 devices implanted per patient. Furthermore, the 30-day all-cause mortality rate in CLASP was low (1.6%; one patient). The death was procedural, as a consequence of a vascular complication at the closure of the femoral access, rather than of the device itself. According to Schäfer, any mortality rate below 5% in a high-risk patient population such as that of the CLASP study is low. He notes all patients, prior to enrolment, were assessed by a multidisciplinary heart team and deemed to be at high risk for surgery.
At the 2019 Transcatheter Valve Therapeutics (TVT) meeting (12–15 June, Chicago, USA), Scott Lim (University of Virginia Health System Hospital, Charlottesville, USA) reported, on behalf of the CLASP study investigators, the six-month results of the CLASP study.3 These showed that the significant reductions in MR seen at 30 days were sustained: at six months 98% of patients had MR grade ≤2+ and 81% had MR grade ≤1+ (Figure 1). Additionally, 88% of patients were in NYHA class I or II and 46% of patients in NYHA class I (these figures were 85% and 37%, respectively, at 30 days) thus showing further improvements; and a significant difference compared with baseline levels (p<0.0001).
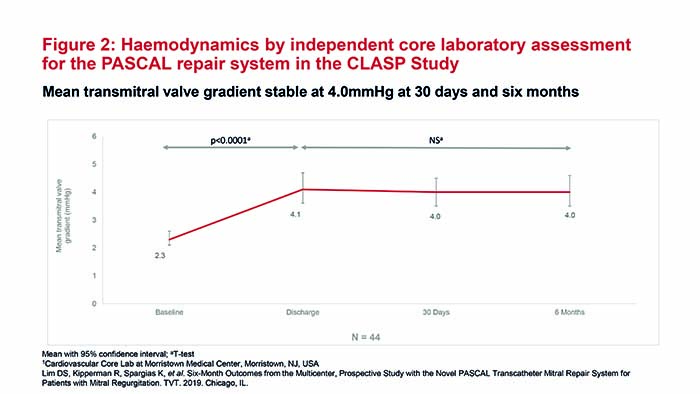
Importantly, mean transmitral valve gradient at 30 days was 4mmHg (p<0.0001 vs. baseline levels) and this result was also sustained at six months (Figure 2), which shows that the PASCAL repair system facilitates leaflet coaptation and wide diastolic openings. Importantly, these results were obtained with 1.5 average devices per patient. Rudolph says: “There is a critical cut-off point when reducing residual flow and, once passed, you are potentially creating a barrier to forward flow—meaning that the heart cannot fill properly with blood. You would expect that if you had a wider device or two devices, if you took more of the leaflets, the risk of such a barrier would be much more likely. With the PASCAL repair system, I think this risk is probably mitigated by the spacer and how it facilitates leaflet coaptation and wider diastolic openings.”
Summing up the data for the PASCAL repair system, Schäfer states: “The outcomes are very convincing. For me, the most striking finding was the very significant reduction in mitral regurgitation.”
Although not explored in the CLASP study, the width of the PASCAL implant may enable operators to only use one device in most cases, and in certain patients with degenerative MR this could be particularly advantageous. Rudolph explains: “In some cases of degenerative mitral regurgitation, getting to all of the diseased parts of the valve can be very challenging. Just imagine if the leaflet is not attached to the chordae in the ventricle, then—in systole—it flips towards the atrial side and it becomes a flail leaflet. Therefore, if it is very wide and you have a narrow device, you might grasp some of it but still have parts that prolapse into the left atrium. But if you have a wider device, achieving maximal coaptation and wider diastolic openings with one device will be much easier.”
In their commentary on the CLASP study, Praz et al write: “The advent of the PASCAL repair system is a welcome addition to the armamentarium of transcatheter mitral valve devices. The early experience attests to the feasibility of the procedure, and further studies will be instrumental to define the appropriate use and indication for this novel device.”4
References
- Lim DS, Kar S, Spargias K, et al. Transcatheter valve repair for patients with mitral regurgitation: 30-day results of the CLASP study. JACC Cardiovasc Interv 2019; 12(14): 1369–78.
- Stone GW, Lindenfeld J, Abraham WT, et al. Transcatheter mitral-valve repair in patients with heart failure. N Engl J Med 2018; 379(24): 2307–18.
- Lim DS, Kipperman R, Spargias K, et al. Six-Month Outcomes from the Multicenter, Prospective Study with the Novel PASCAL Transcatheter Mitral Repair System for Patients with Mitral Regurgitation. TVT. 2019. Chicago, IL.
- Praz F, Windecker S, Kapadia S. PASCAL: A new addition to the armamentarium of transcatheter repair systems for mitral leaflet approximation. JACC Cardiovasc Interv 2019; 12(14): 1379–81.









