
Data from more than 1,000 patients presented during the virtual Society for Cardiovascular Angiography and Interventions (SCAI) 2020 Scientific Sessions (14–16 May, Eastern Time) demonstrates Impella (Abiomed) reduced in-hospital mortality when placed before a non-emergent percutaneous coronary intervention (PCI) is performed. According to a press release, the research found that, in the setting of high-risk PCI, when Impella is placed pre-PCI, it is associated with a 10 times reduction of in-hospital mortality, compared to when Impella is placed during “bailout” PCI.
The data presented were from an adjunct study of PROTECT III; the ongoing, prospective FDA post-approval study for Impella in high-risk PCI. The research is authored by William O’Neill (Center for Structural Heart Disease, Henry Ford Hospital, Detroit, USA) and Jeffrey W Moses (Columbia University Medical Center, New York, USA). They state: “Support with Impella in haemodynamically stable patients undergoing non-emergent PCI, also termed Protected PCI, is now a well-established indication in a selective patient population at high risk for haemodynamic collapse during PCI. However, some physicians may eschew preventive haemodynamic support and prefer a bailout strategy should hemodynamic collapse occur.” The study aimed to quantify the risk of such a bailout strategy.
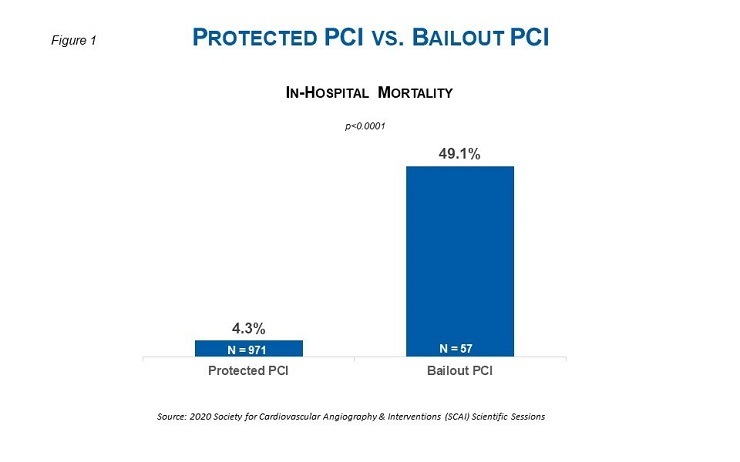
The study analysed 1,028 patients supported with Impella 2.5 or Impella CP (971 in Protected PCI group and 57 in bailout group). In the bailout group, females were more prevalent (50.9% versus 27.2%; p=0.0002), the median baseline left ventricular ejection fraction was significantly higher (40% versus 30%; p<0.0001), heart failure was less prevalent (42.1% versus 56.9%; p=0.039), and left main disease was less prevalent (40.0% versus 56.1%; p=0.03). In summary, the bailout group had a higher percentage of women, the patients were younger, and had a higher ejection fraction with less heart failure. Despite these differences the study found:
In-hospital mortality was significantly higher in the bailout group compared to the Protected PCI group, respectively (49.1% versus 4.3%; p<0.0001). The difference in mortality was significant across patients experiencing haemodynamic collapse secondary to refractory hypotension or coronary perforation/dissection.
O’Neill comments: “Failure to prospectively identify patients who may experience hemodynamic collapse during non-emergent PCI leads to excessive in-hospital mortality. This data shows that Impella support prior to initiation of the PCI can reduce this risk.”









