
Intravascular lithotripsy, or IVL (Shockwave), is a novel procedure that is designed to deliver localised pulsatile sonic pressure waves, modifying calcified lesions in a safe and reproducible manner. In this commentary, Satoru Mitomo, Antonio Colombo, and Azeem Latib explores the need for such a device for treating calcified lesions.
Percutaneous coronary interventions (PCI) with drug-eluting stents are now commonly performed in many types of complex lesions; however, calcified lesions remain one of the most challenging lesion subsets even with current iteration of drug-eluting stents that have thinner struts and biocompatible polymers. To attain the best possible results with drug-eluting stents in calcified lesion(s), appropriate lesion preparation is an essential prerequisite. To facilitate this, devices to modify calcified lesion(s) can be used including cutting/scoring balloons, rotational atherectomy, orbital atherectomy and excimer laser. But for certain types of calcified lesion—eccentric, thick, or deep—the efficacy of these devices is still limited. Furthermore, these devices can be associated with complications including slow/no-flow phenomenon, excessive vessel dissection, or perforation.
The technology of intravascular lithotripsy
The mechanism of intravascular lithotripsy is leveraging electrohydraulic-generated lithotripsy to produce high-speed sonic pressure waves that pass through soft tissue to selectively disrupt calcium. The concept adopted is similar to urologic extracorporeal lithotripsy, but intravascular lithotripsy differs by expressing a field effect of ultra-high energy. It is designed specifically for vascular applications with the technology producing unfocused energy that creates a localised effect only within the vessel.
The system consists of a catheter that houses the emitters and is enclosed in an integrated angioplasty balloon mounted on a rapid exchange system, generator and connector cable. The balloon should be well prepared and inflated with a saline and contrast solution without any residual air.
The balloon size is selected according to the proximal and distal reference vessel diameter. After advancing the catheter to the target lesion guided by radiopaque markers on the catheter, the balloon is inflated at 4atm to contact with vessel wall—facilitating optimal energy delivery. By pushing a button on the cable connected the catheter, the lithotripsy cycle is activated and pulses once per second for ten seconds. After every cycle, the balloon is inflated up to 6atm that compresses the fractured calcium. The cycle is then repeated as needed until the desired lesion expansion is obtained and the maximum repeatable cycle with the same catheter is eight cycles.
Clinical data
The Disrupt-CAD (Disrupt coronary artery disease) study was a prospective multicentre, single-arm study enrolling 60 patients with severely calcified lesions treated with coronary lithotripsy. The main inclusion criteria of the lesions were; severely calcified lesions in a native coronary artery with ≥50% diameter stenosis and >32mm length. The primary performance endpoint was clinical success defined as a residual diameter stenosis <50% following stenting without in-hospital major adverse cardiovascular events (MACE: a composite of cardiac death, myocardial infarction or target vessel revascularisation). The primary safety endpoint was freedom from MACE through 30 days follow-up. The study demonstrated compelling safety and performance results. Intravascular lithotripsy treatment was highly effective in facilitating the delivery of stents and reducing restenosis. Stent deployment was performed in 100% of the patients with reduction in residual stenosis to ≤50% in all patients despite >90% of patients having heavily calcified lesions. There were no major intra-procedural complications including perforation, embolisation, slow-flow or no reflow and a low MACE rate out to six months (8.5%). Consistent, reproducible luminal gain was also achieved. The clinical success rate was achieved in 57 (95.0%) patients, limited only by three (5%) asymptomatic non-Q-wave myocardial infarctions. Catheter delivery and treatment at the target lesion was successful in 59 (98.3%) patients. The primary safety endpoint of 30-day MACE rates was achieved. There were no cardiac deaths, Q-wave myocardial infarction or target vessel revascularisations during this period.
Representative real-world case performed in Milan: Severely calcified lesion treated with intravascular lithotripsy

A 66-year-old male with past medical history of hypertension and dyslipidaemia was admitted with an episode of exertional angina. Coronary angiography revealed a diffusely diseased left main trunk and left anterior descending artery with severely calcified lesions (Figure 1). Preprocedural optical coherence tomography (OCT) showed thick calcification with >180 degrees arc in the lesions (Figure 2).
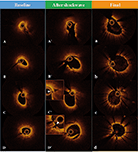
Considering the severity of the calcified lesions, lesion modification with lithotripsy was attempted. According to the OCT measurements, appropriately sized catheters were selected for each segment of the lesions (mid left anterior descending: 2.75mm, proximal left anterior descending to left main trunk: 3.25mm and 3.75mm), and multiple lithotripsies were performed with the methods previously described. Subsequent dilatation with non-compliant balloons facilitated optimal lesion expansion (Figure 1-II) and OCT confirmed cracks of calcification (Figure 2). Three drug-eluting stents were then implanted, followed by high-pressure post-dilatation with NC balloons. Angiography showed excellent angiographic results (Figure 1) and final OCT confirmed symmetric stent expansion and optimal stent apposition (Figure 2).
Future prospects
Intravascular lithotripsy is a unique and attractive technology for the treatment of severely calcified lesions with PCI. Our initial clinical experience with lesion preparation using lithotripsy in real-world complex calcified cases has been promising and associated with efficacy as regards to facilitating stent delivery and ensuring optimal expansion. The potential advantages of this technology as compared to rotational or orbital atherectomy are the ease of use (delivering a balloon to the lesion on any 0.014inch guidewire), short learning curve, less procedural complexity and minimal risk of dissections, slow flow or perforations. A second-generation device with improved crossing profile and deliverability will be available this year. Despite a number of positive attributes, intravascular lithotripsy cannot currently be considered a substitute of rotational or orbital atherectomy because uncrossable lesions will still require a specific atherectomy device to initiate lesion preparation. Further studies are warranted to evaluate this technology in real-world patients, including comparisons with existing technologies. This technology could potentially facilitate and increase the treatment of calcified lesions by many interventional cardiologists that may not be proficient in rotational or orbital atherectomy.
Satoru Mitomo, Antonio Colombo, and Azeem LatibAzeem are all at Interventional Cardiology Unit, San Raffaele Scientific Institute, Milan, Italy











