
This content is only for readers outside of the USA
First real-world case experience with the Cardioband Tricuspid System by Marcel Weber, Jan-Malte Sinning, Nikos Werner and Georg Nickenig.
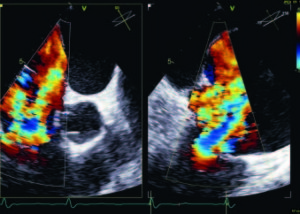


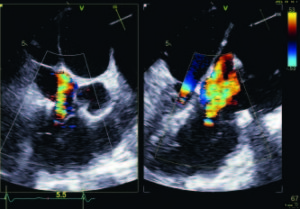
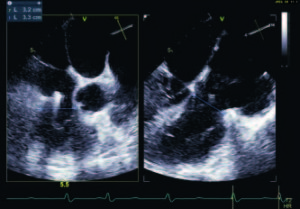
A 78-year-old female presented with dyspnea (NYHA III) and elevated NT-pro BNP level of 526 pg/dl. Three-dimensional transoesophageal echocardiography (TOE) revealed malcoaptation of tricuspid leaflets and massive tricuspid regurgitation (proximal isovelocity surface area [PISA] radius: 9.5mm, mean vena contracta width: 14mm, EROA: 1.2cm², regurgitant volume 105ml/beat, coaptation defect area 2.9cm2, Figure 1) and annular dilatation (septolateral diameter 43mm, anteroposterior diameter 47mm, Figure 1).1 Pre-procedural work-up revealed a non-significant coronary artery disease, a preserved left ventricular ejection fraction (63%) and permanent atrial fibrillation. Concomitant atrial fibrillation is typical in 80% of patients with functional tricuspid regurgitation.2 Six months before, successful mitral edge-to-edge repair was performed to treat severe functional mitral regurgitation. Further comorbidities comprised chronic renal failure stage III (GFR: 57ml/min), pulmonary hypertension (systolic pulmonary artery pressure: 30mmHg) and insulin dependent diabetes mellitus. STS Score and EuroSCORE II were 2.35% and 3.15%, respectively. Prior to the procedure, cardiac computed tomography was used to size the tricuspid annulus for device selection and to plan the procedure (mitigating the risk of injury to the right coronary artery and planning of fluoroscopic views).
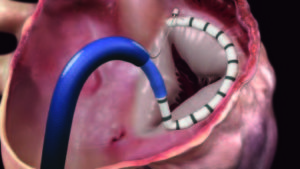

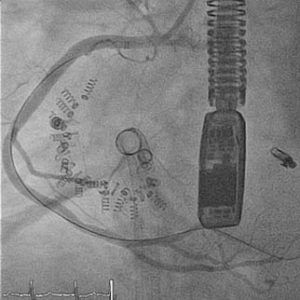
Due to the large coaptation gap and elevated surgical risk, the heart team decided on the Cardioband Tricuspid System (Edwards Lifesciences; Figure 2). The Cardioband Tricuspid System— recently CE mark approved—is a dedicated technology to reduce tricuspid annular dimensions and thus tricuspid regurgitation, similar to the Cardioband Mitral System. The Cardioband implant, which consists of a contraction wire and polyester fabric covering with radiopaque markers attached to an adjustment mechanism, is implanted by a transvenous procedure under echocardiographic and fluoroscopic guidance.

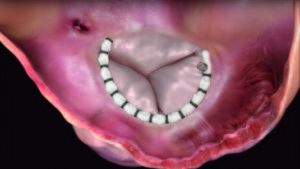
The device is inserted via the femoral vein and advanced to the right atrium to allow deployment from the anteroseptal commissure, in a clockwise direction, to the posteroseptal commissure. Similar to tricuspid surgical repair, the septal portion of the annulus is spared to prevent conduction disturbances. The Cardioband implant was fixed by 17 anchors along the tricuspid valve anterior and posterior annulus. The right coronary artery was accessed with a coronary wire and occasionally coronary angiography was performed to rule out injury to the right coronary artery. After complete anchor fixation of the Cardioband implant, stepwise contraction of the Cardioband was performed under TOE guidance.

Through annular reduction, tricuspid regurgitation severity was reduced from massive to moderate (Figure 3), with a corresponding change in regurgitant volume by two-dimensional PISA method from 105ml/beat to 36ml/beat (Figure 3). PISA radius was reduced from 9.5mm to 4mm, EROA from 1.2cm² to 0.2cm² and mean vena contracta width from 14mm to 4mm (Figure 3). The tricuspid valve septolateral dimension was reduced from 43mm to 32mm with no injury to the right coronary artery (Figure 3).
The patient was discharged home on the fourth postoperative day and TOE prior to discharge confirmed moderate tricuspid regurgitation.
Conclusion
This patient with massive tricuspid regurgitation and high operative risk was successfully treated with the Cardioband Tricuspid System, acutely reducing tricuspid regurgitation severity from massive to moderate. Tricuspid annular reduction using the Cardioband Tricuspid System is an effective and safe treatment option in patients with functional tricuspid regurgitation.
- Hahn et al. The need for a new tricuspid regurgitation grading scheme. Eur Heart J Cardiovasc Imaging 2017; 18: 1342–43.
- Nickenig et al. Transcatheter treatment of severe tricuspid regurgitation with the edge-to-edge MitraClip technique. Circulation 2017; 135: 1802–14.
Marcel Weber, Jan-Malte Sinning, Nikos Werner and Georg Nickenig are affiliated with Heart Center, University of Bonn, Bonn, Germany.






