
This advertorial is sponsored by Shockwave Medical
Coronary artery calcification (CAC) has become increasingly frequent in contemporary coronary intervention driven largely by aging populations, a higher disburden of comorbid conditions and the treatment of long-standing, advanced coronary artery disease.1,2 Approximately a third of all lesions treated with percutaneous coronary intervention (PCI) have significant angiographic calcification which impacts stent delivery and expansion, as well as long term stent outcomes.3-5 Devices designed to modify CAC such as mechanical atherectomy, non-compliant balloons and scoring/cutting balloons can be effective for lesion preparation but have limitations and risks.
Since its introduction in 2021, intravascular lithotripsy (IVL) from Shockwave Medical is an important adjunctive therapy that has become a preferred coronary calcium modification strategy among the interventional cardiology community.6 Recent evidence provides further insight into Shockwave IVL’s mechanism of action as compared to alternative balloon-based strategies. Jason Wollmuth, interventional cardiologist at Providence Heart Institute (Portland, USA) helps to put this new evidence into context and how it has supported and informed his clinical practice during the treatment of CAC.
Why is it important to understand a device’s mechanism of action when thinking about your treatment algorithm?
A better understanding of a device’s mechanism of action helps inform where and when that device should be implemented in clinical practice. There is no “one-size-fits-all” strategy to managing CAC and oftentimes, multiple calcium modification modalities are needed. Utilising intravascular imaging to understand the thickness, length and arc of calcification are important in determining the best approach. Once the lesion morphology is defined, then it is important to understand how each device mechanistically modifies coronary calcification. In balloon uncrossable lesions, an upfront strategy with atherectomy is needed. In balloon crossable lesions, balloon-based strategies are reasonable in calcium less than 0.5mm thick or less than a 180-degree arc. However, in lesions with concentric calcification, calcium that is greater than 0.5mm thick, or an arc of calcium >180 degrees, IVL is a preferred strategy. However, even in vessels with less than 180-degree calcium arc, recent cadaveric studies suggest IVL does reasonably well in fracturing calcium with no medial injury.7 Even in nodular calcium, IVL has been shown to create fractures and thus may be helpful especially in nodules where wire bias doesn’t allow for good contact with atherectomy devices.8 After a calcium modification device is used, it is important to confirm adequate vessel expansion prior to stent implantation. I use a long 1:1 size NC balloon to assess for adequate lesion expansion and intracoronary imaging to assess for calcium fractures.
How would you summarise the mechanism of action of Shockwave IVL?

circumferentially around and longitudinally across
the device
Shockwave IVL uses the energy-based production of ultrasonic acoustic pressure waves—or shockwaves—for modification, fracture, and fragmentation of arterial calcification. Once delivered to a target lesion, the Shockwave IVL balloon catheter is inflated to sub-nominal pressures coupling the balloon to the arterial wall. Shockwaves are produced from electrical energy that travels from the Shockwave IVL generator and terminates at the spark gaps found on the emitters. The energy creates a plasma event which is rapidly absorbed within the fluid-filled balloon and instantaneously produces a Shockwave. Shockwaves travel through soft, non-calcified tissue due to the similar densities of fluid and soft tissue and generate disruptive forces when they encounter a large change in densities as seen in calcium. This minimises vessel injury to non-calcified segments of the artery while maximising fractures in the calcification.
What new evidence provides further insight into Shockwave IVL’s mechanism of action and how it compares to alternative, balloon-based strategies?
medial injury in >50% of histologic sections containing
calcium arcs <180 degrees
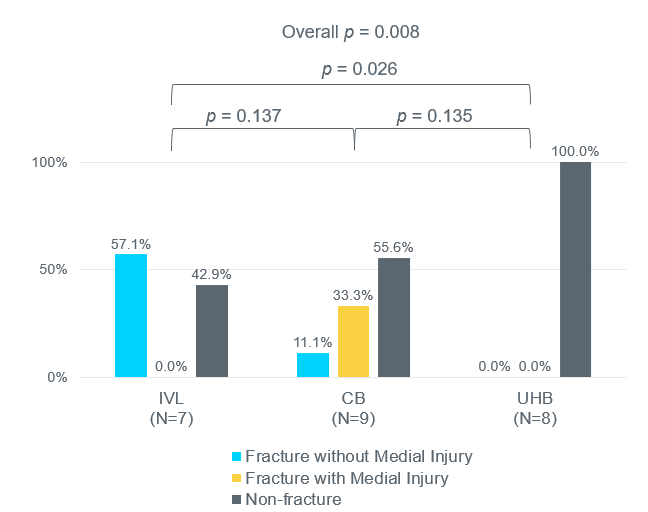
A recent cadaveric study compares the frequency of calcium fracture and presence of medial injury utilising micro-CT and histology within 17 severely calcified lesions treated with Shockwave IVL (IVL), Wolverine cutting balloons (CB) or OPN ultra-high pressure balloons (UHB). Calcium fractures were most frequently observed and medial injury significantly less frequent within lesions treated with Shockwave IVL as compared to CB and UHB. Medial injury occurred in 100% of lesions treated with UHB despite 0.5mm downsizing. Additionally, Shockwave IVL produced calcium fracture with no medial injury in 100% of histologic sections containing calcium arcs ≥180 degrees and within >50% of histologic sections containing calcium arcs <180 degrees. Fractures caused by CB and UHB were mostly associated with medial injury in histologic sections with calcium arcs ≥180 degrees and no calcium fractures were identified within histologic sections containing calcium arcs <180 degrees treated with UHB (Figure 1).7
What are some lesser-known or underappreciated aspects of Shockwave IVL’s mechanism of action that support the findings of this study?
to the emitter at the edge of the treatment zone
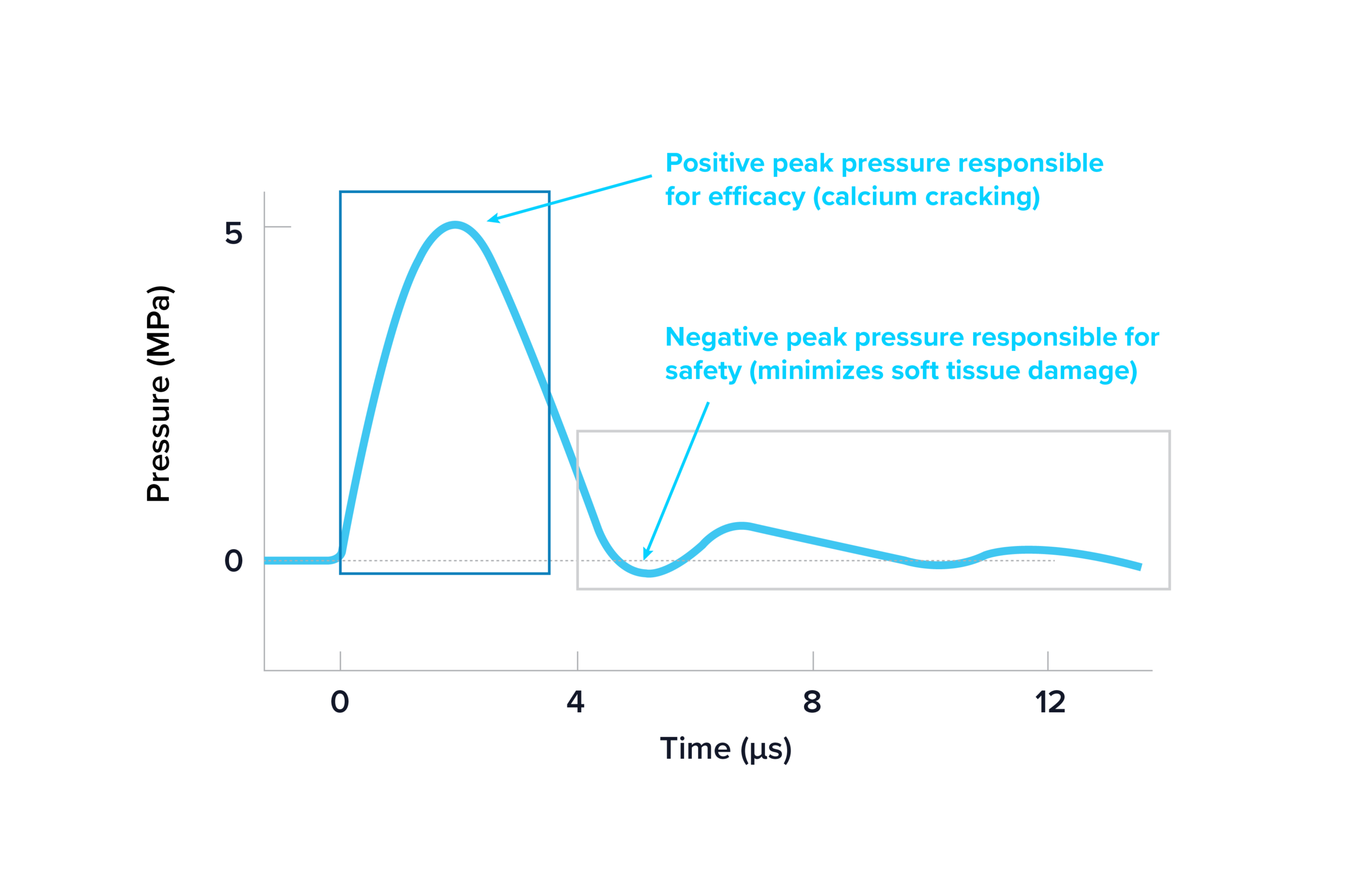
Shockwaves—the ultrasonic acoustic pressure waves produced by Shockwave IVL—consist of an acoustic waveform that is tuned to maximise safety without tradeoffs for efficacy. Perpendicular to the emitters at the edge of the treatment zone, Shockwaves have an acoustic waveform with an average positive peak pressure of ~5MPa (or 50atm) which modify calcium through various forces and an extended duration or low amplitude negative peak pressure which minimises soft tissue damage due to tensile stress.8 The Shockwave acoustic waveform is the basis of the clinical evidence generated to date demonstrating IVL as a safe and effective calcium modification strategy (Figure 2). Additionally, the ultrasonic acoustic output of Shockwaves are measured to be distributed around and across the device. There are no areas between the marker bands or within quadrants around the balloon lacking an acoustic output less than the threshold needed for calcium modification. All together, these aspects of Shockwave IVL’s mechanism of action helps to explain the safety and effectiveness demonstrated in this cadaveric study.
How do the results of this cadaveric study compare to your clinical experience with Shockwave IVL within eccentric calcium?
All calcium modifying devices require contact with the calcific lesion to lead to disruption. Atherectomy devices may miss calcium because of wire bias and scoring/cutting balloons need to have the scoring element in contact with the calcium to lead to disruption. Shockwave IVL’s acoustic output is consistent circumferentially around the balloon and along the length of the balloon which maximises the likelihood of calcium fracture. This fits with clinical experience where Shockwave IVL seems to add value in a variety of calcific lesions. In addition, the low tensile stress (from the propagating shockwave) on soft tissue minimises medial injury that can be seen with other balloon-based strategies.
Any closing remarks?
Shockwave IVL has become an important tool in managing coronary calcification. Its ease of use, safety and efficacy have lead to a rapid uptake in the interventional community and it is now the most commonly employed calcium modification device.6 Understanding its mechanism of action and data from recent cadaveric studies give operators confidence that Shockwave IVL can be effective in managing a variety of calcific lesions.
References
1.CDC. Trends in aging. MMWR Morb Mortal Wkly Rep. 2003;52:101–106.
2.Guzman RJ. Arterial calcification. J Vasc Surg. 2007;45(Suppl A):A57–63.
3.Madhavan MV et al. Coronary artery calcification. J Am Coll Cardiol. 2014;63:1703–14.
4. Généreux P et al. Two-year outcomes after PCI of calcified lesions with DES. Int
J Cardiol. 2017;231:61–67.
5. Généreux P et al. Ischemic outcomes after PCI of calcified vessels in ACS (HORIZONS-AMI & ACUITY pooled). J Am Coll Cardiol. 2014;63:1845–54.
6. Butala NM et al. Use of calcium modification after introduction of coronary intravascular lithotripsy. J Soc Cardiovasc Angiogr Interv. 2024;3(2):101254.
7. Sekimoto T et al. Vascular injury from IVL vs cutting vs ultra-high-pressure balloons. J
Am Coll Cardiol Intv. 2025;18(17):2093–2104.
8. Kereiakes, D, Virmani, R, Hokama, J et al. Principles of Intravascular Lithotripsy for Calcific Plaque Modification. J Am Coll Cardiol Intv. 2021 Jun, 14 (12) 1275–1292.
9. Ali ZA et al. Outcomes of coronary intravascular lithotripsy for calcified nodules (Disrupt CAD pooled). EuroIntervention. 2024;20:e1454–64.
Disclaimer: Jason Wollmuth is a paid consultant of Shockwave Medical, the views expressed are of their own opinions, reflect their daily medical practice and do not necessarily represent Shockwave Medical.
In the USA: Rx Only. Prior to use, please reference Instructions For Use for information on indications, contraindications, warnings, precautions, and adverse events. www.shockwavemedical.com/IFU
Please contact your local Shockwave representative for specific country availability.
SPL-79436 Rev. A










