
This advertorial is sponsored by iVascular
In certain complex percutaneous coronary intervention (PCI) cases where there may be a discrepancy in the diameter of the treated vessel, using a stent that has the ability to adapt to the anatomy of the artery can be advantageous. In this article, Cardiovascular News speaks to Armando Pérez de Prado (University Hospital of León, León, Spain) and Manel Sabaté (Hospital Clinic Barcelona, Barcelona, Spain) who detail when and how stent overexpansion can be deployed to good effect and offer their views on how the overexpansion capacity of the Angiolite (iVascular) drug-eluting stent (DES) make it a useful option in these cases.
“A common challenge in PCI is stent sizing, particularly when there is a large variation in vessel size, for example in left main PCI or aneurysmal coronary arteries,” says Pérez De Prado. In these types of cases, the operator must “push the boundaries of what coronary devices are capable of” to achieve an optimal result, he comments. “Current stent designs have a narrow range, presenting a huge problem in choosing the current stent size, leading to suboptimal stent expansion,” he says of the currently available stent platforms.
According to Sabaté, understanding stent sizing, as well as the ability of the stent platform to adapt to the size of the vessel, are important aspects to take into consideration when choosing a device that suits the specific anatomy of the patient. “It is important to know the diameters of the distal and proximal parts of the segment that we are going to treat, and the type of stent that can accomplish the diameter we need to treat the patient,” he comments.
 There are certain cases where these factors are particularly relevant, Sabaté goes on to explain. “The paradigmatic example to take into account the overexpansion of a stent is the case of a bifurcation,” he says. “You have to know the size of the distal and the proximal segment, and then the capacity of the stent to adapt to either segment.”
There are certain cases where these factors are particularly relevant, Sabaté goes on to explain. “The paradigmatic example to take into account the overexpansion of a stent is the case of a bifurcation,” he says. “You have to know the size of the distal and the proximal segment, and then the capacity of the stent to adapt to either segment.”
Bifurcation cases can pose a challenge due to the difference in diameter between the proximal and distal part of the main branch. Sabaté describes stent overexpansion as being of the “utmost importance” in these cases, particularly when seeking to avoid dissections in the distal part of the vessel and stent under-expansion in the proximal segment. “Left main bifurcations with the left anterior descending (LAD) and circumflex arteries are the paradigm of this issue and the capacity of the stent to adapt to the proximal part of the left main is crucial in this part of the anatomy,” he explains.
PCI in the left main coronary artery may also pose a challenge due to the large diameter of the vessel and the subsequent risk of stent under-expansion, which raises the risk of stent thrombosis and restenosis. This presents another such scenario in which having access to a device with a good overexpansion capacity can prove beneficial.
Turning to their use of the Angiolite stent, both physicians agree that the device is a standout choice in these challenging cases due to the combination of good radial force and overexpansion capacity. Angiolite is a sirolimus-eluting coronary stent composed of alternating links to achieve a homogeneous arterial coverage with high rates of endothelialisation due to a fluorinated polymer and TransferWise, proprietary iVascular nanotechnology.
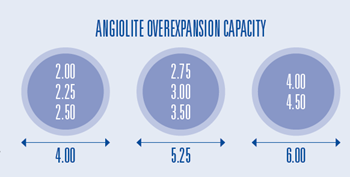
“The Angiolite stent has a unique design to allow overexpansion up to 6mm,” comments Pérez De Prado of the distinct aspects of the device. “The design of the stent with alternate links between the crowns is to allow growing overexpansion of some parts of the stent, without having deformation.”
The overexpansion capacity of Angiolite is 6mm for diameters of 4mm and 4.5mm, whilst for small vessels, from 2mm to 2.5mm, the maximum overexpansion capacity is 4mm. For medium vessels, such as 2.75mm, 3mm and 3.5mm, Angiolite offers 5.25mm as a maximum post-dilatation diameter.
“The Angiolite stent is a very interesting device because it has, on the one hand, a good radial force, and on the other hand a good overexpansion capacity that can overcome all of the issues in bifurcations, in the left main, and when you want to adapt to impact the stent exactly in the proximal end of the left main apposed to the wall and not hanging in the lumen,” says Sabaté. “In my experience for the left main LAD, the left main circumflex situations, the Angiolite is one of the preferred stents for these anatomies.”
“In my experience for the left main LAD, the left main circumflex situations, the Angiolite is one of the preferred stents for these anatomies.”
“When there are big discrepancies of diameters in coronary arteries, one of the most important features to consider for a DES is its overexpansion capacity in order to accommodate the most challenging lesions,” adds Pérez De Prado, who says that Angiolite has shown excellent performance in these challenging settings.
Details
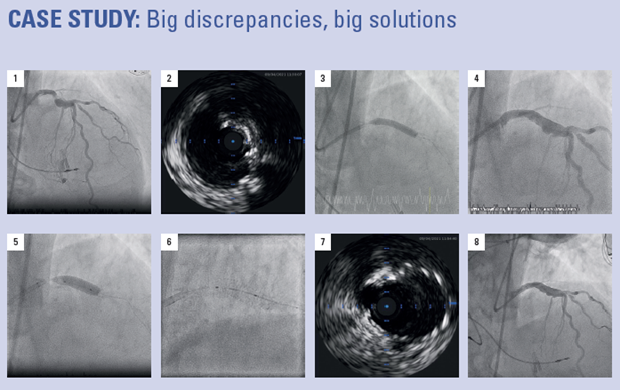
A 78-year-old male was admitted after non-ST segment elevation myocardial infarction (NSTEMI). Angiography showed two-vessel disease with severe calcification and proximal stenosis in the left anterior descending (LAD) artery with a 90-degree bend.
Procedure
1) A radial approach and crossing of the LAD lesion were attempted, but calcification required a switch to a femoral approach. After five attempts to cross the lesion, a guidewire was able to reach the diagonal branch. 2) An intravascular ultrasound (IVUS) run was performed, showing a high degree of severe calcification and severe persisting stenosis. 3) The proximal LAD lesion was dilated with a non-compliant 5mm balloon. 4) An Angiolite 4×24mm was implanted, and IVUS showed significant infraexpansion of the stent. 5) A 6mm non-compliant balloon was used in the proximal part of the stent. 6) The result was significant lumen gain. 7) A 6mm non-compliant balloon was applied achieving lumen gain of this segment. 8) Final assessment showed an excellent angiographic result.









